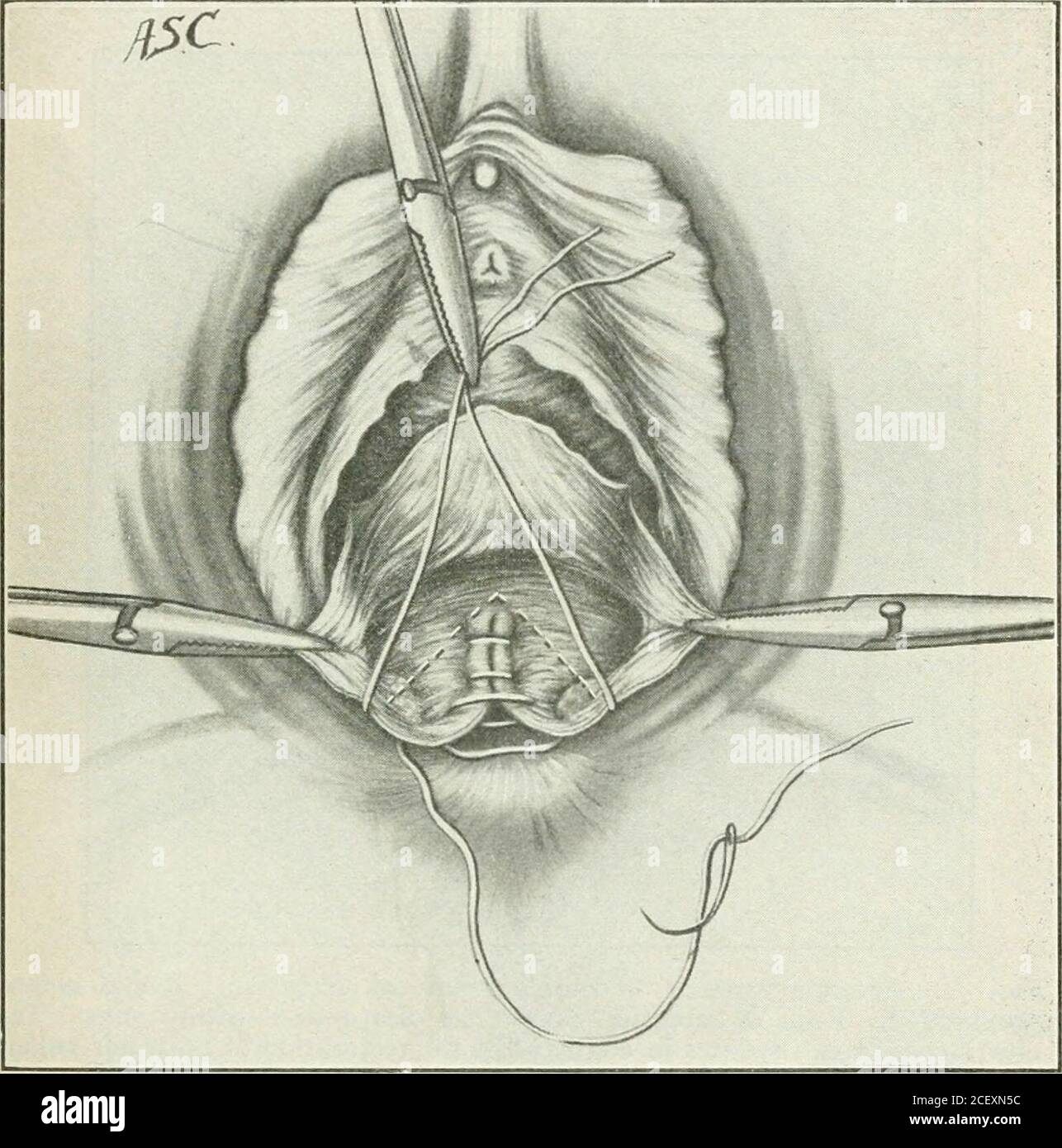
. A manual of gynæcology and pelvic surgery, for students and practitioners. Fig. 69.—Secondary repair of complete perineal laceration. Continuousrectal suture in position but not drawn up. Deep retention suture laid throughsphincter ends. set suture. It is not always feasible to finish and tighten thelowermost end of this suture until a retention suture for thesphincter is placed. This should be of rather coarse silkwormgut and is introduced behind, not through, the ends of the sphinc- ±I!^ltiiNiLW±/Ul!/K.AllUiN b/ ter and passes high up toward the apex of the wound as de-scribed on page 131
{kind=link}
Image details
Contributor:
Reading Room 2020 / Alamy Stock PhotoImage ID:
2CEXN5CFile size:
7.2 MB (347.8 KB Compressed download)Releases:
Model - no | Property - noDo I need a release?Dimensions:
1573 x 1589 px | 26.6 x 26.9 cm | 10.5 x 10.6 inches | 150dpiMore information:
This image is a public domain image, which means either that copyright has expired in the image or the copyright holder has waived their copyright. Alamy charges you a fee for access to the high resolution copy of the image.
This image could have imperfections as it’s either historical or reportage.
. A manual of gynæcology and pelvic surgery, for students and practitioners. Fig. 69.—Secondary repair of complete perineal laceration. Continuousrectal suture in position but not drawn up. Deep retention suture laid throughsphincter ends. set suture. It is not always feasible to finish and tighten thelowermost end of this suture until a retention suture for thesphincter is placed. This should be of rather coarse silkwormgut and is introduced behind, not through, the ends of the sphinc- ±I!^ltiiNiLW±/Ul!/K.AllUiN b/ ter and passes high up toward the apex of the wound as de-scribed on page 131. When drawn upon this suture approxi-mates the ends of the sphincter, and the continuous rectal sutureis tied while the retention suture is held. The latter is thentied and cut and the ends at once retract inside the anus. If. Fig. 70.—Secondary repair of complete perineal laceration. drawn up. Rectal suture deemed necessary one or two fine buried catgut stitches may beapplied in order more closely to unite the sphincter ends. The tear now has been converted into the incomplete formand the final repair is made by suturing the vaginal side of therecto-vaginal septum and the skin surface. 150 INJURIES TO THE PERINEUM AND PELVIC DIAPHRAGM General Remarks.—Though operations upon the femaleperineum are performed in an area which is never completelyor even adequately sterilizable, they are almost uniformlysuccessful if properly performed. Prehminary asepsis neverthe-less should be as perfect as possible. Large preliminary douches, made soapy with green soap, creoHn or lysol should be